|
David Zigmond
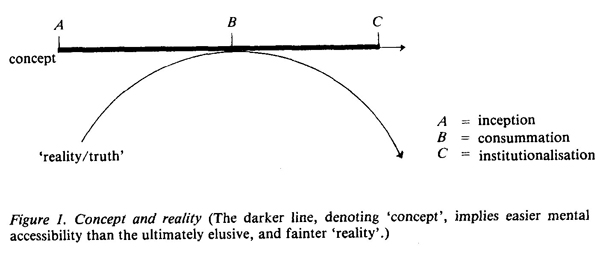
(Erich Fromm, Man for Himself, 1947) Several years ago, an intelligent and troubled friend of mine I shall call her Carol then in her mid-twenties, was sent to a psychiatrist because of worsening symptoms of depression. She remembers him as a kind, fatherly man who asked her a comprehensive range of questions to survey her symptoms, life and dilemmas. Before she left, he informed her of his view that her pattern of distress would be 'best treated by psychotherapy', and that he would make arrangements accordingly. Carol, although a bright and educated young woman, came from a background largely alien to matters psychological and introspective. Her parents, pragmatic Northerners from an industrial city, represented a culture and way of thinking very different from the psychodynamically sophisticated psychiatrist she encountered; she did not know what psychotherapy was and he, perhaps unwittingly, did not explore this gulf between them. It was several weeks before Carol received a standardised letter from the hospital, telling her of an appointment with Dr. L., a psychotherapist, in four months' time. By the time Carol went to see Dr. L. her most troublesome depressive symptoms had largely subsided, perhaps due to medication she had been prescribed. She was, however, left with a churning, ineffable chaos inside her, which became heightened on the day of her appointment; the fantasy of her imminent meeting with Dr. L. produced an added, tense composite of hope and fear. A long period of waiting in a neon lit and threadbare waiting area preceded the appearance of Dr. L. 'Miss Jackson? I am Doctor L. Will you follow me please, was Dr. L's sparse greeting. His voice seemed uncompromisingly dry and neutral, Carol thought, as she was led along a corridor and into a small, bare room in which there were two easy chairs. Dr. L. closed the door behind them and silently gestured to one of the chairs, as he sat down himself. A period of silence followed which, for Carol, was unexpected and increasingly uneasy. Her previous encounters with her own doctor and the psychiatrist had been in some ways embarrassing and difficult, but reassuringly structured by the initiative they took in asking questions, and offering explanations and suggestions of various kinds; at those times she had felt encouraged by the elementary support and interest shown to her. Dr. L., however, seemed quite different with the silence growing laden and unnatural, Dr. L's gaze felt paralysing to Carol, and, when he turned his eyes to the floor, she felt unaccountably abandoned and unsafe. She had wanted to ask him what she was expected to say or do, but became increasingly anxious that she might be breaking some kind of unspoken code by doing so, although part of her was aware of the irrationality of the notion, Dr. L's silence and inaccessibility in the face of her mute need and fear, had turned him, in her mind's eye, into some kind of omniscient and unappeasable giant that she could not now approach directly. Perhaps ten or fifteen minutes passed in this kind of ominous wilderness before Dr. L., shifting slightly in his chair, said rather rhetorically: 'I suppose you're rather angry, but don't know how to express it'. 'Angry, why should I be angry? I just feel rather confused ...' pleaded Carol, disoriented and frustrated, imagining that she had somehow missed her cue, that he demanded some kind of 'correct' response that she had not been able to fathom or, therefore, provide. 'Confusion can be an excellent way of avoiding strong feelings when they seem threatening', came Dr L's reply, authoritative and consummate. But I still don't know what you mean. Who am I angry with?' replied Carol, beginning to find some kind of clarity and confidence, perhaps because this silent and inscrutable man was now, at least, speaking to her. 'Perhaps with the hospital who kept you waiting for an appointment so long. And then, again, with me for keeping you outside (in the waiting area) isn't that what happened in your family, that they kept you "waiting outside, when you were sent to boarding school?' Carol was slightly taken aback by his knowledge of her; again her fantasies turned to his omniscience, and her sense of his having a secret cache of understanding about her, and a hidden agenda with her, to which she was denied access. Bewildered by these potent images, she retreated to the more tangible suggestion that he made: But I understand the NHS system; I know that there are waiting lists for all kinds of services, and that I can't blame anyone for that. Anyway, I have been feeling rather better lately ', said Carol with a mixture of appeasement and defiance. 'Perhaps so, but knowing about things doesn't necessarily make you less angry. Your "feeling better" might also be a way of avoiding angry feelings ,' countered Dr. L. didactically, but not unkindly. Carol felt impotent and at an impasse with Dr. L., and the two again lapsed into a silence, as long and uncomfortable as the one which had preceded it. 'I don't think individual psychotherapy would be suitable for you, but I'll see what the possibilities are for a group that you might be able to attend', Dr. L. informed Carol, indicating that their session and relationship were at an end. Carol sensed, at that time, and a retrospective view indicates her correctness in this, that a group was not what she either needed or wanted. Carol's contact with the hospital was lost. Card was not 'damaged' in any obvious or dramatic way by the failure to develop any rapport with Dr. L., but she reacted by developing a well-articulated suspiciousness of psychotherapy and its practitioners, which, at its sharper end, had a cynical and defiant edge. The blunter aspect revealed a wariness, more vulnerable and afraid. Her symptoms, so deeply rooted in her first and now current relationships, and her internal representations of these, continued a fluctuating but unresolved course. Only in recent times, after talking with me at length about her experience in particular, and the problematic nature of therapy and therapists in general, has she come to modify and destructure her mistrustful view. Now, Carol is not the 'easiest' patient; often feeling threatened and hurt, she has developed a formidable capacity to distract by quips, intellectual commentaries and apparent 'insight' which, in fact, conceals from herself and others what she does not want revealed. These strategies were probably even more difficult to counter when Dr. L. saw her. But she maintains, and I believe her, that even ten years ago she might have been accessible to psychotherapy, had her interview been more geared to making contact rather than interpretations. Let us shift our focus now from Carol to Dr. L. and construct a plausible, if hypothetical, understanding of what he was doing. The evidence, of course, is Carol's, but she is a reliable witness with a good memory and, most importantly, the pattern she describes is too frequent and significant for it to be glibly and technically dismissed, as merely a defensive manifestation of patients' difficulties; there is wisdom as much as hostility in the many bad (and good!) jokes about psychotherapists and analysts. It seems that Dr. L's style was prescriptive and didactic in its process. He presumed a well-defined and elaborated model by which to codify and 'understand' Carol's difficulty. So wedded was he to this model that it automatically led to a 'technique', which he immediately applied; rather than slowly establishing a dialogue, he confronted her from the outset by the paradox of non-contact. The purpose of this, presumably, was to deprive Carol of her usual props and strategies, and via the ensuing anxiety to 'make her aware' of her fear, hostility, manipulativeness, or whatever. We may assume that Dr. L. was working from a psychoanalytic base, where he preconceived Carol's depression as being a consequence of retroflected anger, and that this anger itself is a residuum of her earliest developmental tasks of separating herself from mother, and integrating 'good' and 'bad' objects and feelings. Carol sees now that this kind of understanding has value in making sense of her turbulence, but is certainly not the only, or even the most effective, way of doing so. Other family and social factors have been equally important in leading Carol to her present conflicts and impasse. Dr. L. seems not to have heeded this, however. It is likely that he was a therapist of precise and rigorous training and strong conviction, who 'knew' what her psychopathology was, and the only effective therapeutic stratagem to be applied; all else would be an avoidance or dilution of these central truths. He did not, first, need to make a relationship with Carol, where he could learn about Carol's world in her own language. The important task was that Carol should learn from him, that he should demonstrate quickly and clearly to her the issues she must necessarily confront. He did not require much time to do this; his training had made him skilful and dexterous, and many of his colleagues admired and reinforced his articulate commitment. According to Hannah Segal (1979), Melanie Klein believed that 'things cannot be a bit like this and a bit like that. In matters of science, there can be no compromise...'. While this may be a necessarily pragmatic principle in a Court of Law, where 'truth' must be clear-cut and accessible to bureaucratic process, it is liable to become absurd or sinister when applied to situations that are as complex as understanding human nature. Those scientists concerned with the most precise observations and formulations physicists have long ago given up the search for inviolable truths. Since Einstein and Heisenberg (Einstein & Infield 1938) 'truth' has become relativistic and pragmatic; sometimes it is convenient to consider `matter' as a wave-form, at other times a particle the 'truth' is either, neither, or both of these. The skill of the physicist lies in the sophistication and knowledge behind his 'juggling' with the different models. In the realm of understanding ourselves and our fellows, this relativistic principle is even more important than in physics; our models may have a relation to truth, but they are not themselves 'true' in an immutable sense. We can introduce an illustration (Figure 1) here to clarify this theme:
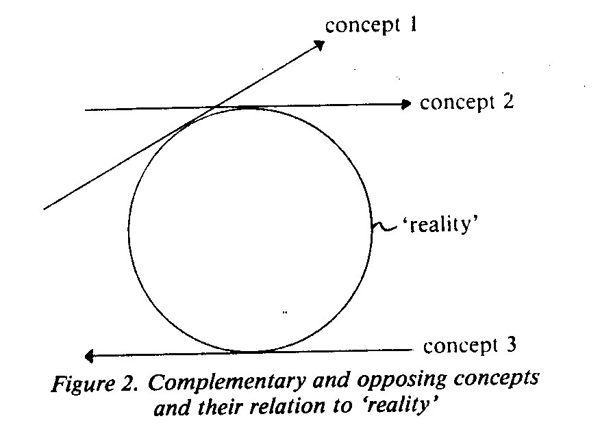
Notice here how the straight line 'concept' touches the curved 'reality' at only one point, B, but that further travelling along the concept departs increasingly from reality. Our psychological formulations often have this quality: we sketch a rudimentary idea, seeing a certain relation to reality, A; as we develop and refine the idea we reach an optimum point, B, of contact with reality, but further thinking along this line departs from it. The process of A>B is disciplined, creative and exploratory, but B>C is increasingly dogmatic, defensive and professionally solipsistic. It is part of the art of psychotherapy to know when 'point B' has been reached, or passed, and to consider another approach. In academic and intellectual circles, ideas are often assessed by logical connection and coherence with other ideas. It is assumed that if a body of knowledge or theory is internally coherent, then it is somehow more true than one with internal discrepancies and contradictions. While such a philosophy has a certain aesthetic appeal, and may keep us in familiar territory, it is no test of the validity of usefulness of an idea. Eastern philosophies have long recognised the fruitfulness and wisdom in reconciling opposites and incongruents (i.e. Yin and Yang of Taoism). Another diagram (Figure 2) illustrates opposing concepts and their relation to reality. If we use this to survey psychotherapy, then concepts 1 and 2 would be closely related approaches, which are complementary and easily reconciled, unless they become institutionalised: an example of this would be Freudian and Kleinian Analytic approaches, both of which stress the importance of discovering or uncovering unconscious and archaic conflict.
Concept 3, however, deals with aspects of reality in a way that is both juxtaposed and in the opposite direction; Glasser's Reality Therapy, which insists on personal responsibility in the present, and regards interpretation as likely to be an avoidance of this, represents such an opposing and incongruent concept. Although widely separated and having opposing vectors, concepts 2 and 3 come closer to resembling a circle than do concepts 1 and 2. Translated back to the realm of psychotherapy, we can see then that a therapist who discriminatingly chooses to work interpretatively from a Freudian base at one time, while at another will not do this but insists that the patient merely look at his actions and their consequences, is closer to the patient's reality (the circle) than the therapist whose eclecticism, for example, extends only to a choice of interpretative frameworks (concepts 1 and 2), or even more than the therapist who has only one conceptual system his choice, then, is limited to how zealously to apply his technique. We can understand Dr. L's professional behaviour as being an example of this. Scientific studies in psychotherapy are concerned with the development of concepts from their inception (point A in Figure 1) to their consummation (point B). Tenacity to concepts beyond this point becomes an issue of institutionalisation or religious conviction, important phenomena which will be discussed later. The art of psychotherapy may be thought of as the ability to draw different tangents at different times, to know when and how diverse forms of understanding and intervention may contact a patient's reality, and how these different lines may connect to make a whole (Figure 3).
Such 'holism', of course, can never be complete, for it would require an infinite number of integrated approaches. However, a large part of our task in being a 'good-enough therapist' consists in having competent and fluent use of a wide variety of ways of understanding. To evoke another metaphor, understanding people who come to us is like musical composition. The composer who knows about only one instrument will be restricted in the sounds he can create. The more he is acquainted with different, sometimes 'opposite', instruments and the relationship between them, the richer and more creative the product. Of course, the composer is thoroughly trained in the use of one instrument first, but it is the transposition of this discipline to other, less familiar, instruments and the learning of the new discipline of 'orchestral holism', which leads to the desired sound. Eclecticism in psychotherapy is often disparaged by more doctrinaire practitioners as being unformed, undisciplined and unfocused. I would maintain a different position: as with the composer, we must first learn one approach thoroughly, and then the fresh task of orchestrating the diverse and the unfamiliar awaits us. Our unwillingness to make this transition may lead us to the limited arena of expert, but stereotyped, performances: we may even institutionalise our performance, and validate our endeavours by having contact only with those professionals who agree with us. As with Dr. L., though, we may develop skills much respected by our ideological cohabitees, at the price of relating to our patients with freshness and creativity; Dr. L. almost certainly had more rapport with his colleagues than with Carol. It is not the psychoanalytic base of Dr. L's practice that is in question here, but the fact that he seemed unable to part from it. With considerable sophistication he had turned a 'base' which allows departure from it into a 'trap' that does not, and to which Carol could respond only by acquiescence or struggle. Such reductionism has earned mental health professionals the title of 'shrinks' who, by inference, reduce patients' human complexity, so that it may become subordinate to the professionals' sphere of influence and explanation. In this regard, psychoanalysis offers to such practitioners the same opportunities and dangers as other 'convergent' modes that have developed well-defined and elaborated systems of language, explanatory theory and professional protocol, for example traditional psychiatry. By contrast, those approaches, which are 'looser', more divergent and have less linguistic or conceptual precision, e.g. Existential or Client-Centred Therapy, would seem freer from this dilemma (though confronted equally by others). As in the realm of physical medicine, techniques and tools that penetrate, define and disable, however briefly, offer their potency inextricably linked with their hazards. Such activities require special capacities of discrimination and responsibility. There arises also the important distinction between 'training' and 'education'. `Training', the more formal and didactic learning process, is almost certainly an important and elementary cornerstone in our development as therapists. The discipline involved in becoming thoroughly and systematically acquainted with one conceptual system is an essential requisite for later, more exploratory, ventures. Just as the infant needs a secure base in a consistent mother, to be able to leave her and relate to others and the vicissitudes of the wider world, perhaps therapists need a 'mother-model' which provides consistent familiarity, before the wider world of psychotherapy, with all its paradoxes, lacunae and frustrations can be confidently and creatively encountered. The process by which we venture away from the `mother-model', and make new and unforeseen contacts and syntheses, is our task of 'education'. There are other interesting and enlightening images we may draw from this metaphor; just as some children have a fearful and insecure attachment to mother, and cannot tolerate separation to make other relationships, so there are therapists who need always to cling to the mother-model, and respond with the many kinds of anger or fear if this is challenged. As the mother-child relationship becomes fixed, so does the therapist-model relationship become institutionalised (as in Figure 1). Dr. L. probably represented this kind of petrified developmental arrest. By contrast, the therapist who is able to internalise a good and consistent mother-model, and confidently but discriminatingly move into new and different therapeutic systems, is like the child who values and trusts his mother, but knows there are other good things for him in the world beyond. `The will to truth is merely the longing for a stable world, Nietzsche (1888) wrote, many years before such matters became psychologically and academically scrutinised. His maxim is particularly relevant to those of us constructing (some might wish to say 'discovering') truths which we then apply to others. Many of us, perplexed and frightened by chaos both within and without, hope that some doctrine religious, psychological, philosophical or political will free us from this tempestuous burden. In recent times, the previously castle-like refuge of religious doctrine has crumbled, leaving psychology and politics, in particular, as ideological havens from a world that can otherwise seem frighteningly outside of our control, purpose and understanding. There are other quasi-religious functions involved: the formation of groups of fellow-believers can imbue members with a sense of mission, enlightenment and righteousness, making outsiders appear in darkest error. Viewed in this way, we can see why the definition and possession of the 'Right Way' in psychotherapy can be such a quirky, often jealous and paranoid business. It accounts also for Carol's first round of experience in this psychotherapy-roulette; she was dealing with Dr. L's credo. From the end of our intra-uterine life onwards, it is a central and never-ending task for each of us to learn to live creatively in the constant shadow of uncertainty. At our beginning, the womb expels us, the 'ideal' mother disappears or disintegrates, younger children unaccountably appear to supplant us. At the other end of our lives, our internal resources become erratic and fail us, friends and loved ones die, often without warning. In the middle is the swirling mosaic of choices, dilemmas and unfinished projects that make up the lot of Man in a rapidly changing world. The task of tolerating and using uncertainty, to open up new possibilities, lies at the heart of sanity, growth and intimate relationships. Whatever formal diagnosis we apply to those who come to us, much of what we deal with are manifestations of disruption in meeting this challenge; we cling to archaic adaptations, notions, feelings and formulae largely because, whatever distress they may cause, they are ways of being that are relatively certain, familiar and predictable. A crucial part of our role as therapists then, if the patient is willing, is to beckon him away from his private but painful base of distorted 'certainty' and, in measures he can tolerate, introduce him to a more unpredictable world in which there are many more possibilities, both in how he perceives himself and how he may relate to others. An important practical question arises from this: how can the therapist who is anxiously and rigidly attached to his mother-model, help the patient abandon his subjective but 'certain' fictions, and journey out into a more real, but more uncertain, world? True, there are equally vital and opposing tasks in psychotherapy. In some situations, if only for short periods, we need to operate with clarity, authority and a large degree of certainty. Just as children, at times, need a parent who is uncompromising and unswerving, so, of course, do patients. The therapist who is unable to do this when it is needed, faces similar long and short-term consequences as the parent who is unable to set firm, clear boundaries and rules. In taking this stance, however, we must satisfy ourselves that it emerges from a substantially considered choice, rather than our own incapacity to encounter the alien and the uncontrollable. Cleverness, often the product of training, is frequently and ritualistically overvalued in our professional culture, and then consists of pursuing a concept or ideology to the limits of sophistication and elaboration, giving an illusion of mastery and command over the unfamiliar. Wisdom, the more delicate child of education, contrasts with, and departs from, such cleverness, and invites us, instead, to enter less charted areas, where the incongruous, the uncertain and the ungovernable await us, and our willingness to acknowledge them. It is perhaps a hallmark of maturity and substance in all our endeavours, to be able to make this kind of transition. References Einstein, A. & Infield, L. (1938) The Evolution of Physics. Cambridge: Cambridge University Press. Nietzsche, F. (1888) The Will to Power. Segal, H. (1979) Klein. London: Fontana. The author is a Senior Lecturer at the North East London Polytechnic and Psychotherapist at the Hammersmith Hospital.
British Journal of Psychotherapy, Vol. 2(4), 1986 Copyright © David Zigmond 1986, 2010 Interested? Many articles exploring similar themes are available via David Zigmonds home page on www.marco-learningsystems.com David Zigmond would be pleased to receive your FEEDBACK
|